Editor's Note: Part 1 of a two-part commentary explains the differences in cloth face coverings and surgical masks, the science of respiratory protection, and the hierarchy of disease controls. Part 2, to be published tomorrow, will outline what makes a good mask study and why so many fail.
Dr Brosseau is a national expert on respiratory protection and infectious diseases and a research consultant with the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota (UMN). Dr Ulrich is a UMN assistant professor in the Division of Environmental Health Sciences and a CIDRAP researcher. Dr Escandón is a physician and infectious diseases researcher in the Division of Infectious Diseases and International Medicine at UMN and also collaborates on research with CIDRAP. Cory Anderson is a graduate research assistant with CIDRAP. Dr Osterholm is CIDRAP director and Regents Professor at UMN.
____________________________________________________________________
Confusion continues to abound over the effectiveness of masks to protect people from COVID-19, and recent news stories touting imperfect studies are only compounding the situation.
First, there was confusion and then intransigence about the modes of transmission, with the US Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) insisting for many months after SARS-CoV-2 emerged that the virus was transmitted only by large droplets or hand contact. Only fairly recently did those agencies finally recognize that inhalation of small infectious particles in the air ("aerosols") is a more important mode of transmission.
That was followed by substantial misinformation and misunderstanding about the role of cloth face coverings, surgical masks, and respirators in preventing SARS-CoV-2 spread. Then we had misunderstandings and poor messaging about the efficacy of different interventions, the effectiveness of one intervention versus another, and why interventions should be considered in a particular order or hierarchy.
In addition, numerous high-profile studies have concluded that face coverings or masks protect against COVID-19, but they often lack scientific rigor, making such conclusions an overreach.
So it is completely understandable that the public and even the scientific community expresses confusion over how well masks protect against a respiratory disease like COVID-19. In part 1 of this commentary we will cut through the murk by: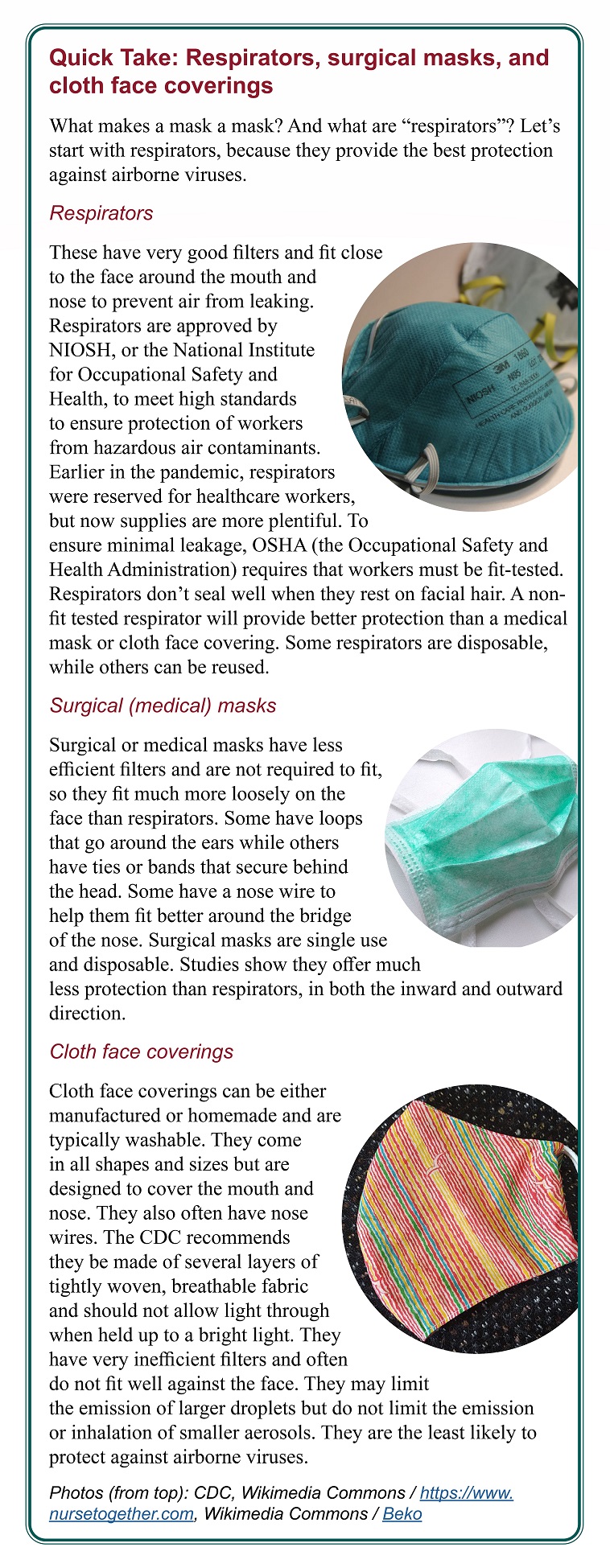
- Explaining the differences between cloth face coverings (or cloth masks), surgical masks, and respirators in the context of infectious aerosol inhalation.
- Delving into the science of respiratory protection.
- Discussing the role of masks and respirators in the hierarchy of controls for disease prevention.
(For simplicity, we will broadly use "masks" to refer to both cloth face coverings and surgical masks, unless this difference is specified. Respirators like N95s are not considered to be masks [see sidebar at right]).
Part 2, to be published tomorrow, will dig deeper by:
- Detailing how the quality of evidence to inform mask policies could be improved via well-conducted studies.
- Laying out—using several recent publications as examples—how to assess studies about masks, underscoring the importance of waiting for the peer review process conducted by subject matter experts before drawing conclusions.
Let's follow the growing body of evidence
It is critical to balance the need for rapid information sharing with rigorous and methodical scientific investigation during a pandemic.1 Early in the pandemic, messaging about masks compromised the latter for the former with the understanding that, with time, more data would become available to make clear the role that masks, in combination with other interventions, might play in limiting person-to-person transmission of SARS-CoV-2.
Now, over a year and a half into the pandemic, we are beyond the initial need to communicate information rapidly as part of the emergency response. Rather than a focus on singular studies, scientists and the media should focus on the growing body of scientific evidence, while at the same time calling for sound study methodologies that advance the science and fill existing knowledge gaps.
At the outset, we want to make clear that we are not "anti-mask." Rather, we are in favor of wearing the most protective facepiece for the setting—such as a non-fit tested respirator when spending more than a few minutes in a crowded indoor space—and in combination with other interventions.
The data are clear that most cloth face coverings and surgical masks offer very limited source control (protection of others from pathogens by limiting emissions from an infected person) and personal protection against small inhalable infectious particles and should not be considered a replacement for other, more effective methods of reducing one's exposure to SARS-CoV-2, such as vaccination and good ventilation.
We strongly support people wearing more effective facepieces, including respirators. Even if not fit-tested, an N95 filtering facepiece respirator (FFR)—or any other respirator—will offer better protection from COVID-19, if sized and worn correctly.2 As there is now ample supply, it is no longer important to reserve respirators for healthcare workers only.
The science behind respiratory protection
Aerosol inhalation requires different interventions
Despite early overwhelming evidence3 that SARS-CoV-2 is transmitted primarily by inhalation of infectious particles in the air (aerosols), it took the WHO and CDC many months to recognize this mode of transmission in their scientific briefs.4,5 Neither agency, however, has adequately directed its guidance away from droplet and contact transmission toward interventions that focus primarily on preventing aerosol inhalation.
Droplet transmission, or propulsion of large particles from sneezing or coughing into the nose, mouth, and eyes of those nearby, could be prevented by erecting barriers between people, physical distancing, and wearing masks with filters that capture large particles. None of those interventions, however, is effective for smaller inhalable particles, which are the predominant size created by people in high concentrations when breathing, talking, singing, etc. Smaller particles stay in the air for long periods (hours), are easily distributed by diffusion and air currents throughout a space (thus negating the effects of physical distancing), and can carry many virions. Masks have filters that do not efficiently capture smaller airborne particles and leave gaps around the mask that allow small particles to leak both in and out.3,6
The interventions that prevent aerosol inhalation are those that reduce the concentration of small particles in a shared space and the time someone spends in that space inhaling those small particles. Particle concentration can be reduced by having fewer people in the space, sharing space for shorter periods, using ventilation that removes particles quickly near the source, and using source controls (masks and respirators) with good filters and fit.
Masks and respirators
Early in the pandemic, CIDRAP published an article describing the differences between cloth face coverings, surgical masks, and respirators.6 The most important features of anything worn on the face to prevent the emission of respiratory particles (source control) or protect the wearer from inhaling infectious particles (personal protection) are filter efficiency, breathing resistance, and fit, in that order.
The CIDRAP article describes appropriate methods for testing these three important variables and the published data for each type of mask or respirator. At that time there were no standards for cloth face coverings and only a small number of surgical masks were tested for filter performance (but not breathing resistance or fit).
Masks generally have very low filter efficiency for small particles, increasing breathing resistance with the addition of more layers of cloth, and very poor fit. Respirator filters, on the other hand, are rigorously tested by the National Institute for Occupational Safety and Health (NIOSH) for filter efficiency and breathing resistance, and the Occupational Safety and Health Administration (OSHA) requires individual fit-testing of a NIOSH-approved respirator before it is worn in the workplace.
There remains no standard method for testing outward leakage (source control) for any mask or respirator. Despite numerous studies throughout the pandemic, very few have used appropriate testing methods.
A 2021 study by Lindsley et al,7 which evaluated outward leakage of a range of face coverings, masks, and respirators on a mannequin, filter efficiency and breathing resistance using appropriate methods, and fit (inward leakage) on human subjects, is perhaps the best recent study to demonstrate the differences between cloth face coverings, surgical masks, and respirators.
In early April 2020, the CDC recommended face coverings in public settings where physical distancing was difficult, suggesting that two layers of fabric worn snugly against the face and secured with ties or ear loops would provide adequate protection.8 The agency, however, did not describe or require any performance tests for filter efficiency, breathing resistance, or fit.
In May 2020, the CDC messaging expanded to "Your cloth face covering may protect them. Their cloth face covering may protect you," implying that everyone would be protected if everyone wore a face covering.9 This message was predicated on the misunderstanding that SARS-CoV-2 was transmitted only by large droplets emitted during coughing or sneezing. In July 2020, based on just two very limited studies in a hospital and hair salon, CDC Director Robert Redfield, MD, touted "Cloth face coverings are one of the most powerful weapons we have to slow and stop the spread of the virus—particularly when used universally within a community setting."10
It was not until November 2020, however, that the CDC finally published a scientific brief on face coverings, which again expanded the message to indicate that they could also protect the wearer from droplets, while finally recognizing that face coverings vary widely in filtration effectiveness.11 The brief fails to recognize or discuss the very limited efficacy of face coverings for preventing the emission or inhalation of small infectious particles and offers no guidance for the assessment of filter efficiency, breathing resistance, or fit.
ASTM, formerly known as the American Society for Testing and Materials, is an international standards organization that develops and publishes voluntary consensus technical standards for a wide range of materials, products, and services. There is now an ASTM standard for barrier face coverings (BFCs).12 A BFC is defined as "a product worn on the face, specifically covering at least the wearer's nose and mouth, with the primary purpose of providing source control and to provide a degree of particulate filtration to reduce the amount of inhaled particulate matter." The standard includes performance tests for filter efficiency and breathing resistance and either qualitative or quantitative assessments of leakage. Lacking a standardized method for evaluating outward leakage (source control), the standard relies on well-accepted fit-testing (inward leakage) methods.
NIOSH, the agency responsible for approving respirators, designated two performance levels for ASTM BFCs used in workplaces13—workplace performance and workplace performance plus—that require, in addition to a high degree of filter efficiency and low breathing resistance, a quantitative assessment of leakage on a panel of human subjects. As of Oct 1, there were 12 ASTM BFCs and 2 Workplace Performance Plus ASTM BFCs listed on the NIOSH Personal Protective Equipment Information website.14
Protection afforded by masks, respirators
ACGIH (formerly the American Conference of Governmental Industrial Hygienists), a professional scientific organization dedicated to advancing occupational and environmental health, created a COVID-19 Task Force in November 2020, which developed several fact sheets for workplace health and safety, including a table that illustrates the degree of protection offered by different types of masks in comparison to a respirator.15 We have modified this table to demonstrate that an N95 FFR, even if not fit-tested, offers more benefits as both source control and personal protection than any mask (Table 1; French translation available here).
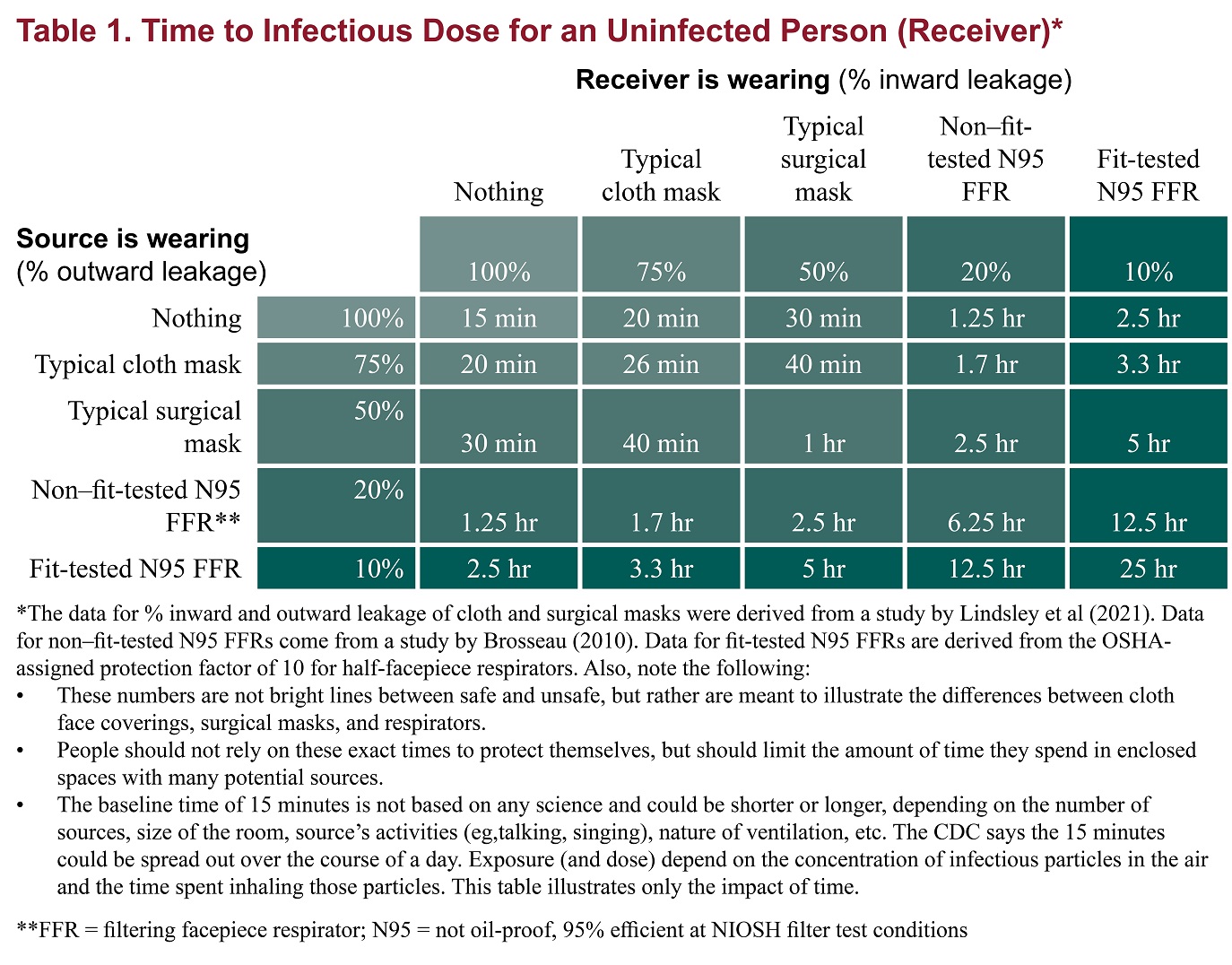
The CDC's 15-minute contact tracing time serves as a baseline for the "time to an infectious dose" when neither the source (infected person) nor the receiver (uninfected person) is wearing a mask or respirator. The time for someone to receive an infectious dose when one or both are wearing a mask or respirator can be calculated by dividing the 15-minute baseline by the percentage of outward leakage (source control) or percentage of inward leakage (personal protection), or both.
(These numbers are just estimates based on the CDC's 15-minute contact tracing time, which has no scientific basis. And the more transmissible Delta variant (lineage B.1.617.2) may require an adjustment to a shorter contact time.)
The receiver's time to an infectious dose increases by a very small amount, to 26 minutes, if both the source and receiver are wearing a typical cloth mask. If both are wearing a typical surgical mask, with 50% inward and outward leakage, the receiver's time to an infectious dose expands to an hour. If both are wearing a non–fit-tested N95 FFR, which will exhibit 20% leakage if sized and worn correctly,2 the time to an infectious dose for the receiver increases to more than 6 hours. If both are wearing a fit-tested N95 FFR, the time to infectious dose expands to 25 hours.
Thus, the public should not rely on typical cloth or surgical masks to offer them much time beyond 15 minutes in a shared space with potential sources, even if others are also wearing masks. Wearing a non–fit-tested respirator allows about an hour of time inside a shared space even if no one else is wearing a mask or respirator.
Unrealistic expectations about masks
Dr. John Snow, who is considered the father of modern epidemiology, was derided and disbelieved for most of his career after he clearly demonstrated that sewage-contaminated water was the source of a large cholera outbreak in London. Ironically, people believed that "bad air" (or miasma) was responsible for the disease, despite data demonstrating otherwise. Today we understand the importance of safe water supplies. Snow's story illustrates both how easy it is for unproven beliefs to take hold and how difficult it can be to change long-standing dogmas even when presented with data showing otherwise.
Scientists, journalists, and the public all hope, with very limited evidence, that transmission will be stopped by wearing a couple of layers of cloth with poor filter efficiency in public settings. They ignore evidence of significant transmission in households and workplaces,17–20 where people spend long periods in close contact with others.
Infection depends on the organism's infectious dose (number of virions that lead to an infection), host factors (eg, age, sex, comorbidities), and environmental factors that affect virus viability (eg, humidity, temperature).21 People's dose is a function of personal exposure, which includes both the time they spend in a shared space with one or more infectious people and the concentration of infectious particles in the air of that shared space.
It is understandable that masks have come to play an outsized role in people's minds, because they appear to offer a relatively easy solution that, unlike other interventions, does not significantly interfere with everyday activities. It is easy to see whether someone is wearing a mask, and it is easy to blame the people who do not for spreading infection.22 Mask wearing (or the lack thereof) provides an easy target for blame, when there are many less observable or measurable variables that could be responsible for infection.
Also, it is easier to require people to wear masks in comparison to other, more effective interventions, such as vaccination, limiting the number of people or the time they spend in a shared space, or improving the ventilation in that space. Wearing masks provides an oversized illusion of control over a difficult-to-contain and still largely unknown disease.
The hierarchy of disease control
Public health guidelines have emphasized throughout the pandemic that preventing infection and transmission requires a combination of interventions.23,24 It is important to consider interventions in the context of a hierarchy, from most to least effective (Table 2).
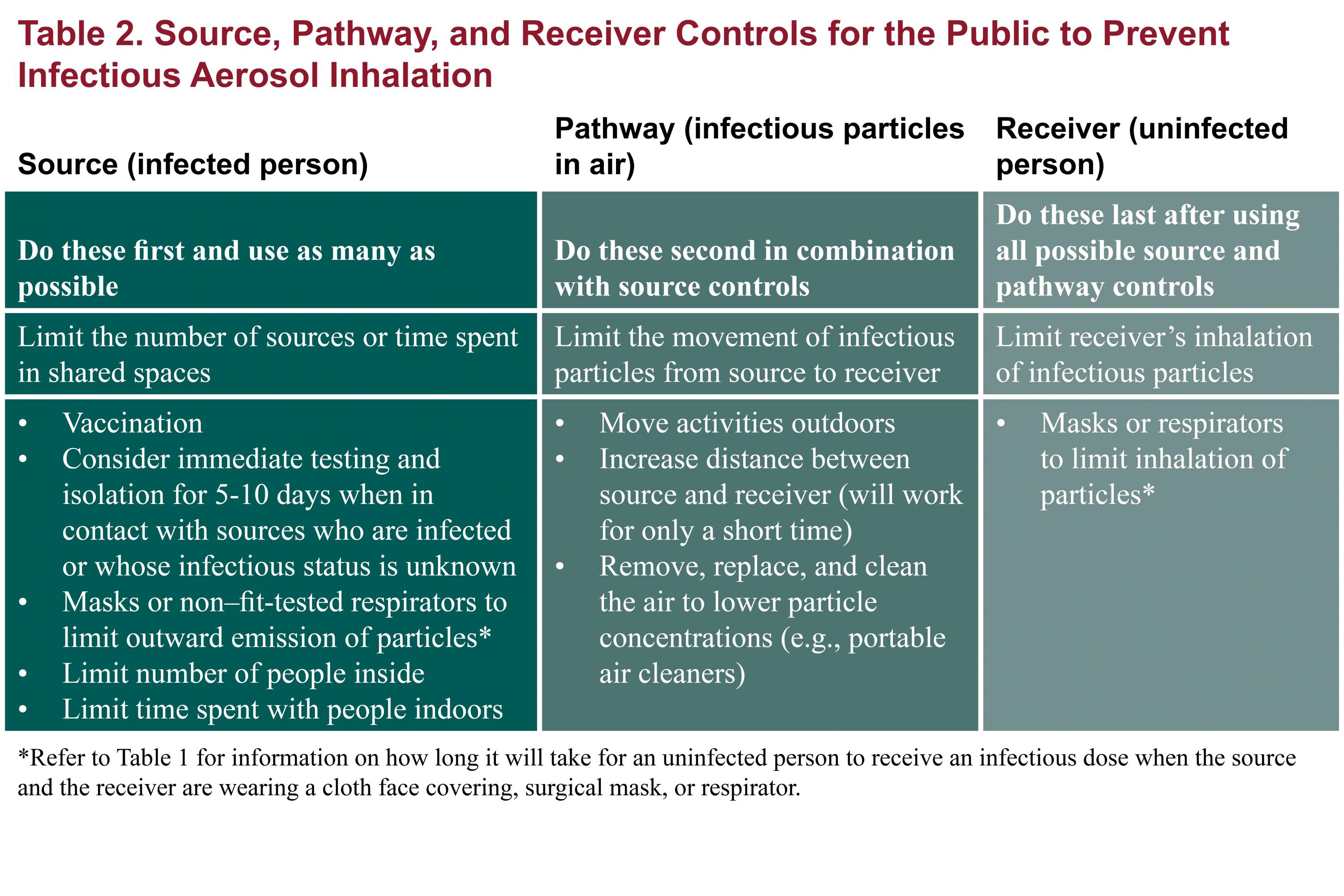
 The most effective interventions are those that eliminate or minimize sources of infection (i.e., infected people), such as vaccination (which lowers the chance of someone being infected),25 limiting the number of people in a shared space (which lowers the likelihood of more than one person being a source), and limiting the time spent in a shared space (which lowers the concentration of infectious particles generated by an infected person).
The most effective interventions are those that eliminate or minimize sources of infection (i.e., infected people), such as vaccination (which lowers the chance of someone being infected),25 limiting the number of people in a shared space (which lowers the likelihood of more than one person being a source), and limiting the time spent in a shared space (which lowers the concentration of infectious particles generated by an infected person).
Ventilation can also be an effective intervention, because it dilutes and removes inhalable particles from a shared space.26 It may not be effective, however, if many sources share a space for a prolonged period.
Cloth and surgical masks offer a very limited degree of source control, because, while they limit the number of larger respiratory particles in a space, they do not prevent the emission of most small particles (aerosols) exhaled during breathing, talking, singing, coughing, or other respiratory actions. Because masks offer limited source control and much more limited personal protection, their effectiveness can be improved only by combining them with other interventions.
At the bottom of the hierarchy of controls is personal protection, such as respirators like N95 FFRs, which can be effective at protecting the wearer, but rely on appropriate fit and consistent wear.
None of these interventions, absent eliminating contact with other people, is effective on its own. But the greater the number of interventions implemented, the lower the risk of person-to-person transmission.22 Some interventions, such as vaccines, are more effective than others, such as masks. As discussed above, anyone wearing a mask should be aware that the longer they spend in a shared space with other people, the greater the risk of being infected.
(Part 2 of this commentary can be found here.)
References
- Sarkki S, Niemela J, Tinch R, et al. Balancing credibility, relevance and legitimacy: A critical assessment of trade-offs in science-policy interfaces. Sci Public Policy 2014 Apr 1;41(2):194-206
- Brosseau LM. Fit testing respirators for public health medical emergencies. J Occup Environ Hyg 2010 Sep 30;7(11):628-32
- Brosseau LM. COMMENTARY: COVID-19 transmission messages should hinge on science. CIDRAP 16 Mar 2020. Available from: https://www.cidrap.umn.edu/news-perspective/2020/03/commentary-covid-19-transmission-messages-should-hinge-science
- CDC. Scientific brief: SARS-CoV-2 transmission. Updated 7 May 2021. [cited 2021 May 8]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html
- WHO. Coronavirus disease (COVID-19): How is it transmitted? Updated 30 Apr 2021. [cited 2021 May 1]. Available from: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-how-is-it-transmitted
- Brosseau LM, Sietsema M. COMMENTARY: Masks-for-all for COVID-19 not based on sound data. CIDRAP 1 Apr 2020. Available from: https://www.cidrap.umn.edu/news-perspective/2020/04/commentary-masks-all-covid-19-not-based-sound-data
- Lindsley WG, Blachere FM, Beezhold DH, et al. A comparison of performance metrics for cloth masks as source control devices for simulated cough and exhalation aerosols. Aerosol Sci Technol 2021 Oct 3;55(10):1125-42
- CDC. Use of cloth face coverings to help slow the spread of COVID-19. 3 Apr 2020. Available from: https://web.archive.org/web/20200404022142/https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html
- CDC. Use of cloth face coverings to help slow the spread of COVID-19. 23 May 2020. Available from: https://web.archive.org/web/20200601211900/https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html
- CDC. CDC calls on Americans to wear masks to prevent COVID-19 spread. 14 Jul 2020. Available from: https://www.cdc.gov/media/releases/2020/p0714-americans-to-wear-masks.html
- CDC. Science brief: Community use of cloth masks to control the spread of SARS-CoV-2. 20 Nov 2020. Available from: https://web.archive.org/web/20210326012539/https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html
- ASTM. ASTM F3502 - 21. Standard specification for barrier face coverings. Available from: https://www.astm.org/Standards/F3502.htm
- NIOSH. Making masks for the workplace. Interim guidance from NIOSH on new masks which build upon the ASTM International (ASTM) standard for face coverings. 18 May 2021. Available from: https://www.cdc.gov/niosh/topics/emres/pandemic/default.html
- NIOSH. Barrier face coverings and workplace performance/performance plus masks. 30 Jul 2021. Available from: https://wwwn.cdc.gov/PPEInfo/RG/FaceCoverings
- ACGIH. COVID-19: Workers need respirators. Available from: https://www.acgih.org/covid-19-fact-sheet-worker-resp/
- OSHA. Assigned protection factors. 24 Aug 2006. Available from: https://www.osha.gov/laws-regs/federalregister/2006-08-24
- Cevik M, Marcus JL, Buckee C, et al. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission dynamics should inform policy. Clin Infect Dis 2021 Jul 30;73(S2):S170-6
- Koh WC, Naing L, Chaw L, et al. What do we know about SARS-CoV-2 transmission? A systematic review and meta-analysis of the secondary attack rate and associated risk factors. Leekha S, editor. PLOS One 2020 Oct 8;15(10):e0240205
- Madewell ZJ, Yang Y, Longini IM, et al. Household transmission of SARS-CoV-2. JAMA Netw Open 2020 Dec 14;3(12):e2031756.
- Althouse BM, Wenger EA, Miller JC, et al. Superspreading events in the transmission dynamics of SARS-CoV-2: Opportunities for interventions and control. PLOS Biol 2020 Nov 12;18(11):e3000897
- Brosseau LM, Escandón K, Ulrich AK, et al. SARS-CoV-2 dose, infection, and disease outcomes for COVID-19—a review. Clin Infect Dis 2021, in press
- Escandón K, Rasmussen AL, Bogoch II, et al. COVID-19 false dichotomies and a comprehensive review of the evidence regarding public health, COVID-19 symptomatology, SARS-CoV-2 transmission, mask wearing, and reinfection. BMC Infect Dis 2021 Dec 27;21(1):710
- Honein MA, Christie A, Rose DA, et al. Summary of guidance for public health strategies to address high levels of community transmission of SARS-CoV-2 and related deaths, December 2020. MMWR Morb Mortal Wkly Rep 2020 Dec 11;69(49):1860-7
- Christie A, Brooks JT, Hicks LA, et al. Guidance for implementing COVID-19 prevention strategies in the context of varying community transmission levels and vaccination coverage. MMWR Morb Mortal Wkly Rep. 2021 Jul 27;70(30):1044-7
- Mostaghimi D, Valdez CN, Larson HT, et al. Prevention of host-to-host transmission by SARS-CoV-2 vaccines. Lancet Infect Dis Sep;2021 Sep 14 (Epub ahead of print)
- WHO. Roadmap to improve and ensure good indoor ventilation in the context of COVID-19. 1 Mar 2021. [cited 2021 Mar 30]. Available from: https://www.who.int/publications/i/item/9789240021280